Dr. Hani Bazzi
Restorative & Aesthetic Dentistry
Institutional Thinking. Long-Term Discipline.
Choose your entry point.
Clinical background, credentials, and documented outcomes
Decision frameworks and treatment logic
Clinical cases, structured and documented.
Positioning
Restorative and aesthetic dentist with over twenty-five years of continuous clinical practice, operating within a structured model focused on long-term functional outcomes rather than isolated procedures.
Clinical Orientation
-Full-mouth rehabilitation-Complex restorative cases-Implant-supported restorations-Interdisciplinary treatment planning
Operating Approach
Clinical decisions are not made in isolation, but within a structured treatment framework designed to ensure:-predictability-functional stability-long-term outcome integrity
Experience
Private Dental Practice — 2001–Present
Lebanese Army — Dental Service — 2000–2001Practicing since 1999
Education
DDS — Tishreen University 1999
Restorative & Aesthetic Dentistry — USJ [2012]
Oral Surgery & Implantology — USJ [2013]
DEA in Oral Biology — Lebanese University [2013]
Contact
Beirut, Lebanon
+961 3 658 929
For a deeper understanding of the framework behind this work:
→ View Professional Philosophy
If this direction aligns with your expectations, I prefer direct and focused communication.
Decision Architecture
My practice is built on one principle:Long-term sustainability is built on structure, discipline, and continuity — not skill.
Over more than twenty-five years in a volatile environment, I have developed an operational model based on:-scientific rigor
-continuous recalibration
-intentional continuityStability is not circumstantial.
It is constructed.
I began practicing at a time when stability was never guaranteed.
Early on, it became clear:Clinical competence alone is insufficient.
Without structure, even strong systems collapse under pressure.
A decade later, I returned to university.
Not to compensate.
To rebuild.This decision redefined how I think, plan, and execute.
Working outside the local context — particularly in Iraq in 2016 — redefined my operational perspective.A clinic is not a place.
It is a system.A system either absorbs pressure — or fails under it.
What followed — economic collapse, pandemic, energy crisis, and war — were not interruptions.
They were stress tests.At each stage, the decision was binary:retreat
or recalibrateI chose recalibration.
Over time, my focus shifted from managing a clinic to designing an operating model built for long-term sustainability—one that evolves through continuous education, critical self-review, and disciplined refinement of standards.Stability is not circumstantial.
It is the outcome of intentional, sustained decisions.My career has not been shaped by volatility, but by the consistency of direction within it.
If you have reached this point, it may suggest that the ideas presented here resonate beyond surface interest. That alignment is often where meaningful collaboration begins.
If this direction aligns, I prefer direct and focused communication.
Clinical Case Framework
Case 01 — Structural Rehabilitation
Phase 1 — Initial Condition

Anterior segment with:
missing central incisor
compromised adjacent restorations
gingival inflammation
Phase 2 — Problem

Not a missing tooth.
A localized structural failure within an unstable environment.
Phase 3 — Transitional

Treatment structured as a sequence:
stabilization
evaluation
integration
Phase 4 — Final Integration

Anterior continuity restored.Note
-The visual improvement is immediate.
-The structural correction sustains it.
Case 02 — Full Anterior Reconstruction
Phase 1 — Initial Condition

Severe anterior breakdown with:
multiple failing restorations
discoloration and structural loss
gingival instability
Phase 2 — Structural Exposure
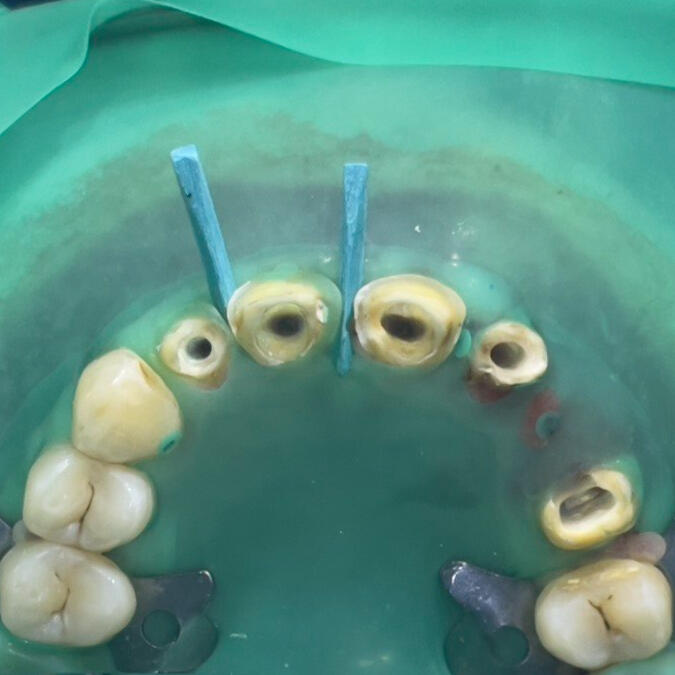
Not a cosmetic issue.
A multi-layer structural collapse requiring full control of the field.
Phase 3 — Controlled Reconstruction

Reconstruction executed as a controlled sequence:
stabilization
structural redefinition
prosthetic integration
Phase 4 — Final Integration

Anterior harmony restored.---Note
-The result appears simple.
-The correction was not.
Case 03 — Anterior Composite Reconstruction (Optical Layering)
Phase 1 — Initial Condition

Fracture of tooth #11 disrupting:
incisal continuity
edge morphology
optical balance within the anterior segment
Phase 2 — Shade Calibration

Shade was not selected from a guide.
It was calibrated in situ.
Composite sample placed directly to evaluate:
value
translucency
interaction with adjacent tooth
Phase 3 — Layered Reconstruction

Reconstruction executed using controlled layering:
opaque layer → structural masking
body composite → natural dentin simulation
high translucency layer → enamel effect
Note
The objective was not to rebuild the tooth.
It was to reconstruct how light interacts with it.